Supplement Testing:
Have We Been Doing it Wrong All These Years?
![]() Michael Lebowitz, D.C. & Noah Lebowitz, D.C.
Michael Lebowitz, D.C. & Noah Lebowitz, D.C.
Abstract
Supplement testing with
applied kinesiology has been a big part of many physicians’ practices, not to
mention all the poorly trained lay people who profess to do applied
kinesiology. The realization that some products can yield hypertonic reactions
has complicated things. The issues are much more involved than even that.
Without trying to unsort these reactions, it can be very easy to prescribe a
supplement that “facilitates” an inhibited muscle but is actually
contra-indicated. We tested 27 patients in various ways to explore this
phenomenon.
Introduction
For decades it has been
the norm in many muscle testing based practices to prescribe supplements.
Besides case histories, laboratory tests, etc., muscle testing is used to help
determine what to prescribe. A supplement is often given that conditionally
facilitates an indicator muscle. Another way to prescribe is to give a
supplement that negates a positive finding be it a therapy localization (TL) to
an organ, a particular muscle inhibition, negates a substance that inhibits
etc. In the year 2011 Dr. Michael Lebowitz and Dr. Ami Kapadia co-wrote a paper
for the ICAK-USA Proceedings entitled Food Toxins. Dr. Lebowitz had observed
that many times a substance someone was sensitive to would make a normally
responding muscle become “hypertonic” (the spindle cells would not “turn off”
when being approximated) and in some patients this was more common than having
an indicator muscle become conditionally inhibited. Upon further testing it was
observed that this held true for nutritional supplements as well as foods
(potentially any substance can do this). Using this finding we found many more
foods the patient could not tolerate and eliminating the foods temporarily and
treating the findings yielded improved patient outcomes.
The following year Dr.
Lebowitz observed while testing under the south pole of a magnet over GV-20
that if a substance yielded a hypertonic reaction and you left it there for ten
seconds that the hypertonicity would turn into an inhibitory response. Dr.
Lebowitz (having never taken a post grad neurology course) hypothesized that
the original hypertonicity was likened to a sympathetic overload response,
which would soon be exhausted and lead to the inhibition of the indicator
muscle. Dr. Sheldon Deal has taught that these hypertonic findings more often
occur with foods a patient is physiologically “addicted” towards.
When it came to
supplements this put us in a quandary. If we were just testing a pure herb
powder it was simple. What if we tested a B Complex or a multivitamin or an
herbal mixture? Let us say for example the supplement has 10 ingredients and
three of them cause a facilitated muscle to become inhibited, three cause an
inhibited muscle to facilitate and four cause hypertonicity. As a result how
would that product test on a patient? Could it test positive while in reality
the patient still might react poorly since 3 ingredients were contraindicated?
Even worse, what about a
four ingredient product where two of the substances cause hyper tonicity and
two cause inhibition? Is it possible the hypertonicity and the inhibition might
cause the facilitation of an inhibited indicator muscle? To us the thought
seemed very plausible that the combo of hypertonic causing ingredients and inhibiting
substances might give you an intermediary response of a facilitation. If so, we
can make many mistakes in our prescribing. Would this hold true in both oral
testing and magnet testing? How can we accurately access the need for
multi-ingredient supplements when this phenomenon exists?
The fact that the
hypertonic reaction turns to an inhibitory response after approximately 10
seconds gave us a clue on how to make this determination. If we have a
supplement that either negates a positive reflex (eg.
inhibition to a TL to one of Chapman’s reflexes negated by a multi-ingredient
vitamin C) or negates a positive substance (eg. blocks
the inhibition to ammonia) or facilitates an inhibited indicator muscle (eg. inhibited pectoralis sternal facilitated by B Complex)
will that finding change if we either leave the substance in the patients mouth
for 10 seconds or leave them exposed to it under a magnet for 10 seconds? If so
should we be waiting that long on all patients before performing the test?
We decided to take a
random group of 27 patients to see if the above mentioned theory is true.
Methods and Procedure
Patients were randomly tested on four substances either under a magnet on
GV-20, orally in ones mouth, or both. They were tested in the offices of Dr.
Michael Lebowitz in Honolulu, HI or of Dr. Noah Lebowitz in Scottsdale, AZ. The
four substances being tested were:
1.
Pure 100% Camu berry
powder.
2.
A multivitamin containing vitamin A, vitamin C,
vitamin D, vitamin E, Thiamin, Riboflavin, Niacin, B6, Folate, B12, Biotin,
Pantothenic Acid, Calcium, Iodine, Magnesium Citrate, Zinc, Selenium,
Manganese, Chromium, Molybdenum, Potassium, Choline Citrate, Boron, &
Vanadium.
3.
A multivitamin protein powder containing vitamin A,
vitamin C, vitamin D, vitamin E, Thiamin, Riboflavin, Niacin, B6, Folate, B12,
Biotin, Pantothenic Acid, Calcium, Phosphorus, Magnesium, Zinc, Selenium,
Manganese, Chromium, Molybdenum, Potassium, Glycine, Medium Chain Triglycerides,
L-Glutamine, L-Lysine, Quercetin, Taurine, MSM, Betaine
Anhydrous, N-Acetyl-L-Cysteine, Choline Citrate, Glutathione, Green Tea
Extract, Boron, Vanadium, Pea protein, Rice Protein, Molasses, Rice bran, monk
fruit, vanilla, and orange flavoring.
4.
An anti-microbial containing Deglycyrrhizinated
Licorice (DGL) extract, Bentonite Clay, Bismuth Citrate, and Berberine.
Each substance was tested on a patient after finding an inhibited
division of the pectoralis major muscle. If the muscle was facilitated by any
of the substances the spindle cells were immediately approximated to check and
see if the substance elicited a hypertonic response. If the substance did not
cause a hypertonic response then the patient was continuously exposed (orally
or via a magnet) for 10 seconds, and then re-tested. These results were written down and
calculated.
Results
Twenty-six patients were tested on the multivitamin with 12 (46%) showing
a positive response (indicator muscle becoming facilitated). Of the 12 positive
tests two of the tests were a hypertonic result. After exposing the substance
to the patient for 10 seconds the patient was re-tested and seven of the
initial 12 people’s indicator was no longer facilitated, returning to its
initial inhibited state. Of the initial 12 positive tests, only five (19%)
remained.
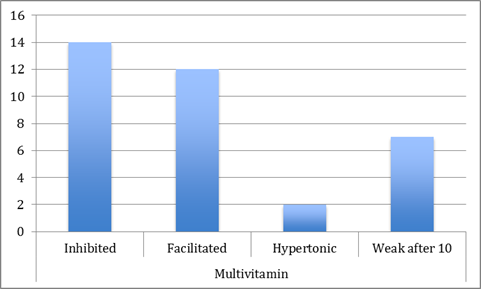
Figure
1 The results are shown of 26
patients tested on a multivitamin
Twenty seven patients were tested on the protein powder/multivitamin with
14 (52%) showing a positive response (indicator muscle becoming facilitated).
Of the twelve positive tests three of the tests were a hypertonic result. After
exposing the substance to the patient for 10 seconds the patient was re-tested
and 10 of the initial 14 people’s indicator was no longer facilitated,
returning to its initial inhibited state. Of the initial 14 positive tests,
only four (15%) remained.
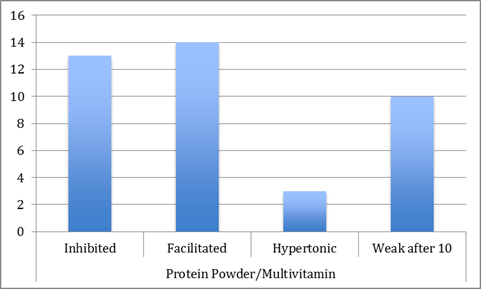
Figure
2 The results are shown for 27
patients checked on a protein powder/multivitamin
Twenty six patients were tested on the antimicrobial with 11 (42%)
showing a positive response (indicator muscle becoming facilitated). Of the
eleven positive tests one of the tests was a hypertonic result. After exposing
the substance to the patient for 10 seconds the patient was re-tested and 8 of
the initial 14 people’s indicator was no longer facilitated, returning to its
initial inhibited state. Of the initial 11 positive tests, only three (12%)
remained.
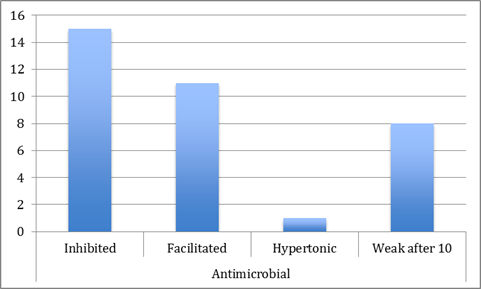
Figure
3 The results are shown for 26
patients checked on an antimicrobial
Twenty two patients were tested on the camu with
13 (59%) showing a positive response (indicator muscle becoming facilitated).
Of the twelve positive tests zero of the tests were a hypertonic result. After
exposing the substance to the patient for 10 seconds the patient was re-tested
and zero of the initial 13 people’s indicator was no longer facilitated,
returning to its initial inhibited state. Of the initial 14 positive tests, all
14 remained facilitated.
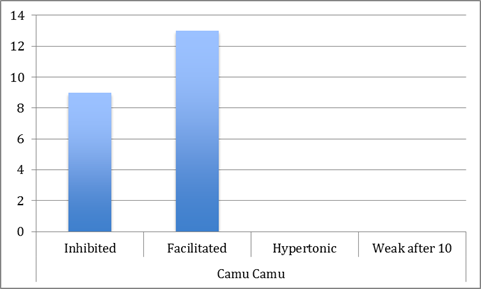
Figure
4 The
results are shown for 22 patients checked on camu
Conclusion
A quick initial glance at the data may make one
wonder of the validity of MMT and nutritional supplementation. In actuality
though, it may mean we have been getting false positives for many years when
testing multi-ingredient supplements. A person tested on the multivitamin may
have a severe Vitamin A and Vitamin C deficiency but have a sensitivity to
artificial chromium and boron. The patient may be in such need of Vitamins A
and C that the supplement initially tests positive. Similar to how sugar will
strengthen people with hypoglycemia, even though it could exacerbate their
adrenal fatigue. We hypothesize that the initial facilitation was due to the
need of certain nutrients, but once the body was able to process the good and
bad, the re inhibition of the indicator muscle showed the presence of the “bad”
components.
Certain single foods
(caffeine, albumin, zein, solanine, etc.) have
previously been shown to cause hypertonicity, which will turn weak after 10
seconds. If an individual food or herb (with no fillers) does not cause hypertonicity,
then the indicator muscle will facilitate if the person needs the supplement.
It will not become inhibited after 10 seconds, as it does with some multiple
ingredient supplements. This was demonstrated by testing camu on patients, which revealed no false
initial positives. The test was either facilitated or not, unlike the three
other mixes, with no change after 10 seconds.
While it does take more
time to screen products this way, the authors recommend all nutritional
supplements which have multiple ingredients should be tested initially and then
re-tested after the patient has been continually exposed to the substance for
10 seconds. This will help us know when to test the individual ingredients of a
multi-product supplement to give our patients the most benefit without any of
the possible negative consequences of prescribing bad along with the good.
References
1.
Lebowitz, Michael DC and Ami Kapadia MD, Food Toxins,
2011 Proceedings of the Annual Meeting, ICAK-U.S.A.
2.
Deal, Sheldon D.C. N.D., Presentation, ICAK-USA Annual
Meeting, Washington
DC, June 2014.